

Advanced Treatments for Depression: What You Need to Know
TL;DR:
- Advanced treatments for depression, such as ECT, TMS, and ketamine, target treatment-resistant cases unresponsive to standard therapies. Neuromodulation options vary in invasiveness and speed, with ECT being most effective but most intensive, while TMS and TBS offer outpatient convenience with quicker sessions. Emerging biological and integrative therapies, including anti-inflammatory treatments and psychedelic-assisted therapy, show promising potential for personalized care approaches.
Advanced treatments for depression are clinically recognized interventions designed for individuals whose symptoms have not responded to standard antidepressants or psychotherapy. These include electroconvulsive therapy (ECT), transcranial magnetic stimulation (TMS), ketamine-based medications, and emerging biological and integrative therapies. The formal clinical term for the population these treatments serve is treatment-resistant depression (TRD), defined by at least two failed antidepressant trials of adequate dose and duration. If you have been through medication after medication without real relief, these options exist and they are backed by growing evidence.
What are the main neuromodulation therapies and how do they work?
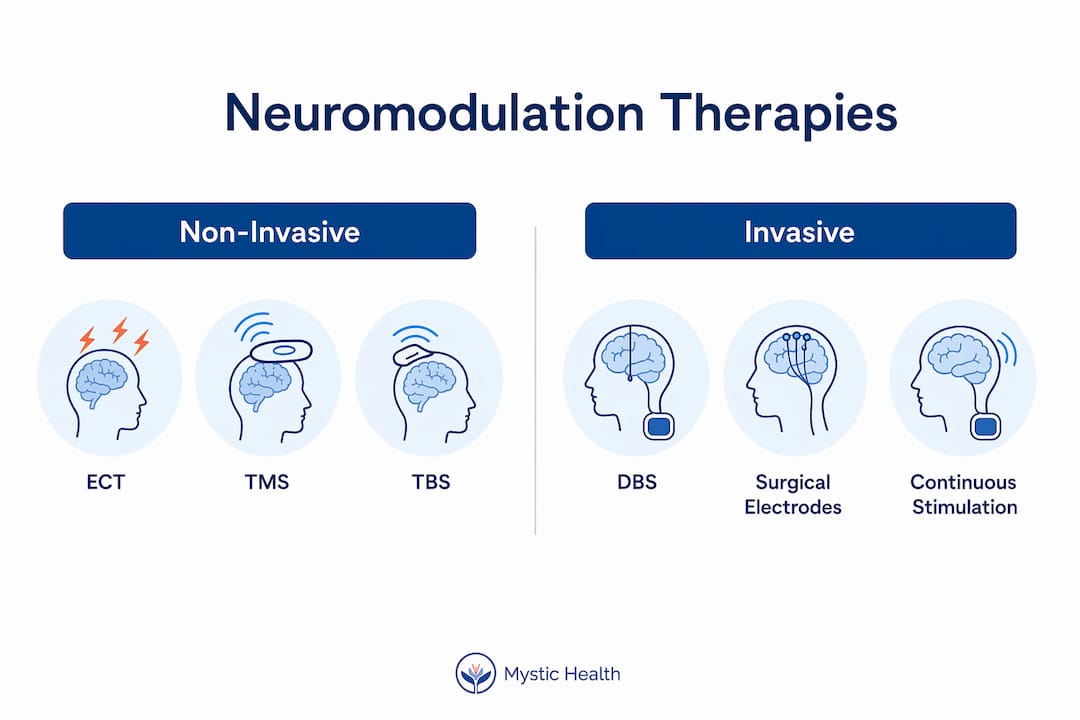
Neuromodulation therapies use electrical or magnetic energy to directly alter brain activity in regions associated with mood regulation. They represent a category beyond traditional antidepressants, offering options that do not rely on daily oral medication and can produce results in weeks rather than months.

ECT (Electroconvulsive Therapy) remains the most effective neuromodulation option available. A 2024 network meta-analysis of 69 trials involving over 10,000 participants confirmed ECT at the top of the efficacy ranking for treatment-resistant depression. It requires general anesthesia and is typically administered in a hospital setting, which makes it the most intensive option on this list. Memory loss is a real side effect, though it is usually temporary.
TMS (Transcranial Magnetic Stimulation) and its faster variant, theta burst stimulation (TBS), are outpatient procedures that use magnetic pulses to stimulate specific brain regions. TBS matches rTMS in efficacy while cutting session time significantly, making it more convenient for people managing work or family schedules. The Mayo Clinic notes that TMS is reserved for people who have not improved with medications, and it carries far fewer side effects than ECT.
Deep Brain Stimulation (DBS) is a surgical intervention involving implanted electrodes that deliver continuous electrical stimulation to targeted brain circuits. It is the most invasive option and currently reserved for the most severe, chronic cases where all other treatments have failed.
| Treatment | Invasiveness | Setting | Session length | Key consideration |
|---|---|---|---|---|
| ECT | High | Inpatient | 15-30 min | Most effective; memory side effects |
| rTMS | Low | Outpatient | 30-40 min | Standard; well-tolerated |
| TBS | Low | Outpatient | 3-10 min | Noninferior to rTMS; more convenient |
| DBS | Very high | Surgical | Ongoing | Last resort; severe TRD only |
Pro Tip: Ask your psychiatrist specifically whether you qualify for TBS rather than standard rTMS. The clinical outcomes are comparable, but the shorter session time can make a meaningful difference in your ability to complete a full treatment course.
How do ketamine and esketamine nasal spray treat depression?
Ketamine works differently from every antidepressant you have likely tried. Traditional antidepressants target serotonin, norepinephrine, or dopamine systems and take weeks to build effect. Ketamine acts on glutamate receptors, producing rapid antidepressant effects that some patients notice within hours of a single infusion. This speed of action is clinically significant for people in acute distress.
Esketamine, marketed as SPRAVATO by Janssen Pharmaceuticals, is the FDA-approved nasal spray formulation derived from ketamine. It carries a specific indication for treatment-resistant depression in adults. The dosing schedule involves twice-weekly administration during a 1 to 4 week induction phase, followed by individualized maintenance dosing. This structure means treatment is not a one-time event but an ongoing protocol managed with your care team.
Here is what the SPRAVATO treatment process typically looks like:
- You arrive at a certified healthcare facility and self-administer the nasal spray under clinical supervision.
- You remain monitored for at least two hours post-dose due to risks of sedation and blood pressure changes.
- You cannot drive yourself home. Transportation arrangements are required for every session.
- Your provider assesses your response and adjusts maintenance frequency based on symptom trajectory.
- Ongoing monitoring continues throughout the maintenance phase to track both efficacy and safety.
The REMS program compliance required for esketamine means it can only be dispensed in certified healthcare settings. This is not a prescription you fill at a pharmacy and take at home. That supervised structure is part of what makes it safe, and it also means you need to plan your schedule around treatment days.
Pro Tip: Before your first esketamine session, arrange transportation in advance and plan for a low-demand day afterward. Many people feel dissociated or fatigued post-dose, and having space to rest rather than returning to work makes the experience more manageable.
For a detailed look at what to expect session by session, Mystic’s SPRAVATO treatment guide walks through the full process from intake to maintenance.
What are emerging biological and integrative therapies?
The latest treatments for depression are beginning to move beyond brain stimulation and glutamate pathways into biology-based and whole-person approaches. These are not yet standard of care, but the evidence is building in ways that are hard to ignore.
-
Inflammation-targeted therapy: A pilot randomized controlled trial from the University of Bristol tested tocilizumab, an anti-inflammatory drug, in 30 patients with treatment-resistant depression who had elevated inflammation markers. The remission rate was 54% with tocilizumab versus 31% with placebo. This matters because it suggests a biological subtype of depression driven by immune dysregulation, one that standard antidepressants may simply not address. Blood tests for inflammatory markers like C-reactive protein may eventually become part of depression workups.
-
SAINT (Stanford Accelerated Intelligent Neuromodulation Therapy): SAINT is a high-dose, accelerated TMS protocol delivered over five days rather than the typical four to six weeks. Remission rates up to 79% within a month have been reported, making it one of the most promising rapid-acting neuromodulation protocols in development. It is not yet widely available, but academic medical centers are expanding access.
-
Psychedelic-assisted therapy: Psilocybin and MDMA-assisted therapies are in late-stage clinical trials for depression and PTSD respectively. Research on psychedelic therapy outcomes shows meaningful response rates in populations that have not benefited from conventional treatment.
-
Integrative mental health approaches: Combining advanced medical treatments with psychotherapy, mindfulness, nutrition, and sleep optimization is not a soft add-on. It is a clinical strategy. Integrative mental health care addresses the full person, not just the symptom cluster, and evidence supports better long-term outcomes when biological treatment is paired with structured psychological support.
These approaches share a common thread: they recognize that depression is not a single disease with a single mechanism. Matching treatment to biology and lived experience is where the field is heading.
How do advanced treatments compare in effectiveness and patient experience?
Choosing among advanced depression treatments is not purely a clinical decision. It involves your schedule, your tolerance for side effects, your access to specialized facilities, and how quickly you need relief.
The 2024 network meta-analysis provides the clearest head-to-head picture available. ECT leads on efficacy for treatment-resistant depression. Ketamine and esketamine follow closely, with the added advantage of rapid onset. TMS and TBS are effective, well-tolerated, and accessible in outpatient settings without the logistical demands of esketamine or the intensity of ECT.
Onset of effect is a critical differentiator. ECT and ketamine can produce noticeable changes within days. Standard TMS typically requires two to four weeks of daily sessions before meaningful improvement appears. SAINT compresses that timeline to five days but is not yet widely available. For someone in acute distress, this timeline difference is not a minor detail.
Tolerability matters too. Neuromodulation therapies like rTMS and TBS are better tolerated than antipsychotic augmentation strategies, which carry risks of metabolic side effects and tardive dyskinesia with long-term use. Esketamine’s dissociative effects during sessions are transient, but they require the supervised setting described above.
Clinicians typically sequence these options based on severity, urgency, and patient preference. Someone with acute suicidality may be directed toward ECT or ketamine first. Someone with moderate TRD who needs to maintain a work schedule may be a better candidate for outpatient TMS or TBS. The clinical evidence base for each of these options continues to grow, and the conversation with your provider should be a two-way one.
Pro Tip: Before your first appointment with a specialist, write down every antidepressant you have tried, the dose, how long you took it, and why you stopped. Confirming true treatment resistance requires a careful medication history, and having this ready saves time and helps your provider recommend the right next step.
Key takeaways
Advanced treatments for depression are most effective when matched to the individual’s biology, treatment history, and practical circumstances rather than applied in a one-size-fits-all sequence.
| Point | Details |
|---|---|
| Confirm treatment resistance first | At least two failed adequate antidepressant trials are required before pursuing advanced interventions. |
| ECT leads on efficacy | A 2024 meta-analysis of 69 trials confirmed ECT as the most effective option for treatment-resistant depression. |
| Esketamine requires supervised settings | SPRAVATO is administered in certified facilities with mandatory post-dose monitoring and no self-driving. |
| Emerging therapies show real promise | Tocilizumab achieved 54% remission vs. 31% placebo in inflammation-positive TRD patients in a pilot trial. |
| Integrative care improves outcomes | Pairing advanced medical treatments with psychotherapy and lifestyle support produces better long-term results. |
What I have learned from watching people navigate these options
By Kabir
I have spent years sitting with people who came to advanced treatments feeling like they had already failed. They had not. The system had just not found the right match yet. That distinction matters more than any clinical protocol.
What I have seen consistently is that the patients who do best are the ones who come prepared. They know their medication history. They have had honest conversations with their providers about what “not working” actually looked like. They understand that treatment-resistant depression is a diagnosis that requires confirmation, not just a feeling. Careful patient history before pursuing advanced options is not bureaucratic gatekeeping. It is how you avoid spending months on a treatment that was never the right fit.
I am genuinely hopeful about where this field is going. SAINT’s five-day protocol, inflammation-targeted treatments, and the growing body of evidence around psychedelic-assisted therapy all point toward a future where we stop treating depression as one disease and start treating it as many. The integrative approaches, the ones that hold space for the whole person alongside the biology, are where I have seen the most durable change. Not just symptom reduction. Actual transformation.
If you are reading this and you are exhausted from trying things that have not worked, I want you to hear this directly: there are still options. Real ones. And the conversation with a specialist who knows this territory is worth having.
— Kabir
Explore advanced depression care at Mystic Health
Mystic Health specializes in exactly the kind of care described in this article. The programs combine esketamine therapy, psychedelic-assisted treatment, and integrative mental health approaches in a supervised, compassionate clinical environment. If you have tried standard antidepressants without lasting relief, Mystic’s team can help you understand which advanced options fit your history and your life. Every treatment plan is built around you, not a protocol. Explore Mystic’s psychedelic and integrative programs to learn what personalized advanced care actually looks like, and schedule a consultation when you are ready to take that next step.
FAQ
What qualifies as treatment-resistant depression?
Treatment-resistant depression is defined by the failure of at least two antidepressant trials of adequate dose and duration. Confirming this history carefully is required before pursuing advanced interventions.
Is esketamine the same as ketamine?
Esketamine (SPRAVATO) is a nasal spray formulation derived from ketamine, FDA-approved specifically for treatment-resistant depression. It shares ketamine’s rapid-acting mechanism but is administered in certified healthcare settings under clinical supervision.
How long does TMS treatment take to work?
Standard rTMS typically requires two to four weeks of daily outpatient sessions before meaningful improvement appears. SAINT, an accelerated TMS protocol, has shown remission rates up to 79% within a month when delivered over five days.
Can advanced depression treatments be combined with therapy?
Yes, and combining them produces better outcomes. Integrative approaches that pair medical treatments like TMS or esketamine with structured psychotherapy and lifestyle support are associated with more durable recovery than either approach alone.
Are inflammation-targeted treatments for depression available now?
Tocilizumab and similar anti-inflammatory treatments for depression are currently in clinical trial stages. A pilot trial showed 54% remission in patients with elevated inflammation markers, but larger trials are needed before this becomes standard care.
Recommended

Mystic Health Blog







FAQs
1. Am I eligible for ketamine therapy?
2. Does insurance cover the cost of ketamine therapy?
3. How many ketamine treatments will I need?
We recommend two initial treatments to determine suitability and adjust dosage. After these sessions, additional treatments are available based on your progress and specific requirements.
