

What Is Dual Diagnosis Treatment? A Clear Guide
TL;DR:
- Dual diagnosis treatment involves integrated care for co-occurring mental health and substance use disorders from the start. It is essential because treating only one condition increases the risk of relapse and hospitalization. Fully integrated programs yield the best retention and recovery outcomes.
Dual diagnosis treatment is defined as the simultaneous, integrated care of co-occurring mental health and substance use disorders within a single, unified clinical framework. Treating both conditions at the same time is not optional. Approximately 50% of individuals with a severe substance use disorder also experience a severe mental illness. That overlap means treating only one condition almost guarantees the other will pull a person back. SAMHSA and leading clinical guidelines recognize integrated treatment as the standard of care, precisely because the two disorders feed each other in ways that separate programs cannot address. If you are researching what is dual diagnosis treatment for yourself or someone you love, this guide walks you through every step.
What is dual diagnosis treatment and how is it assessed?
Accurate diagnosis is the foundation of effective co-occurring disorder care. A clinician cannot build a treatment plan for two conditions if one of them goes undetected.
Standard intake assessment includes a full medical history review, a physical exam, and lab work to rule out medical causes for psychiatric symptoms. From there, clinicians use DSM-5 structured interviews alongside validated screening tools. The PHQ-9 screens for depression severity. The GAD-7 measures anxiety. Both tools give clinicians a quantified baseline that guides medication and therapy decisions.
One of the most underappreciated challenges in dual diagnosis assessment is diagnostic overshadowing. Diagnostic overshadowing occurs when one disorder masks or distracts a clinician from properly identifying the other, which leads to under-treatment of the hidden condition. A person presenting in acute alcohol withdrawal, for example, may have their depression dismissed as a side effect of drinking rather than recognized as a separate, treatable illness.
Pro Tip: Ask your intake clinician directly whether they screen for both mental health and substance use disorders at the same time. If the answer is no, seek a program that does.
The dual diagnosis definition is broader than most people expect. The “dual” in dual diagnosis is an umbrella term covering any combination of substance use and mental health disorders, not just two specific conditions. A person could carry diagnoses of PTSD, alcohol use disorder, and generalized anxiety disorder all at once, and all three require attention from the start.
What treatment models are recommended for co-occurring disorders?
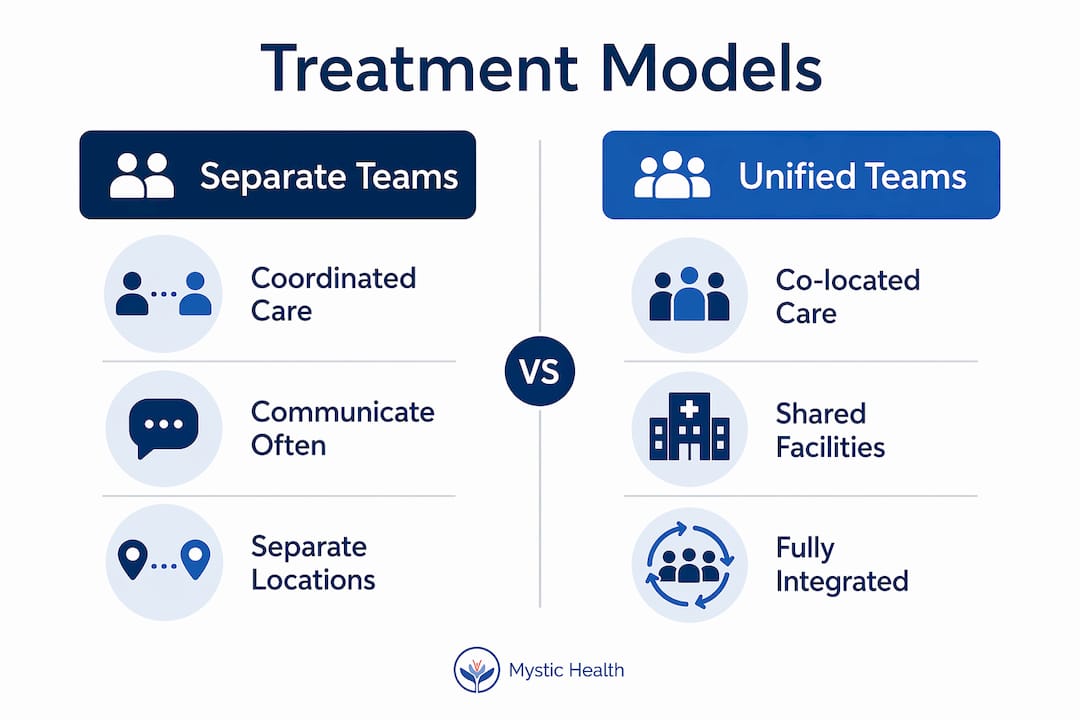
SAMHSA identifies three primary integrated care models for treating co-occurring disorders: coordinated, co-located, and fully integrated care. Each model represents a step closer to unified treatment.

Coordinated care
Coordinated care means separate mental health and substance use teams communicate and share information, but they operate in different settings. It is better than no coordination, but gaps in communication still create risk.
Co-located care
Co-located care places both teams under the same roof. Patients see a psychiatrist and an addiction counselor in the same building, which reduces the burden of navigating multiple systems. Records are more likely to be shared, and warm handoffs between providers become routine.
Fully integrated care
Fully integrated care is the gold standard. One multidisciplinary team manages both conditions simultaneously, with shared records, joint treatment planning, and coordinated medication management. Integrated dual diagnosis programs report the highest treatment retention, the lowest relapse rates, and the fewest psychiatric hospitalizations compared to parallel or sequential treatment. That outcome gap is significant. It means the model of care matters as much as the specific therapies used.
Key advantages of fully integrated care include:
- Shared electronic health records across psychiatric and addiction providers
- Joint medication management to prevent harmful drug interactions
- Unified treatment goals agreed upon by the full clinical team
- Single point of contact for the patient, reducing administrative burden
- Consistent messaging across all providers to reinforce recovery
Programs that function under one clinical umbrella with shared records and joint teams consistently outperform fragmented treatment setups. The evidence for this is not subtle.
Why integrated treatment is essential for dual diagnosis recovery
Fragmented care is not a neutral alternative to integrated treatment. Treating mental health and substance use disorders by separate teams is a documented barrier to recovery that leads to worse outcomes, higher relapse rates, and more hospitalizations. When a psychiatrist and an addiction counselor do not communicate, they may prescribe medications that interact dangerously, or send contradictory messages that undermine a patient’s confidence in treatment.
“Patients with dual diagnosis often manage complex polypharmacy requiring coordinated medication management to avoid dangerous interactions. Psychiatric medication management alongside medication-assisted treatment for substance use must be carefully coordinated. Without that coordination, the risk of harmful drug interactions rises significantly.”
The “no wrong door” policy addresses this directly. It means a patient should never be told to get sober before receiving mental health care, or to stabilize their mental health before entering addiction treatment. Both conditions must be treated concurrently from the first point of contact. This policy reflects a clinical reality: you cannot fully treat depression in someone who is actively drinking, and you cannot sustain sobriety in someone whose untreated anxiety drives them back to substances.
Pro Tip: When evaluating a program, ask whether they treat both conditions from day one. Any program that requires you to “complete” one treatment before starting the other is not practicing integrated care.
Early detection and integrated treatment significantly increase the chances of lasting recovery and reduce hospitalizations. The sooner both conditions are identified and addressed together, the better the long-term prognosis. This is not just clinical optimism. It reflects what the data consistently shows across treatment populations.
What to expect in dual diagnosis programs and levels of care
Dual diagnosis programs exist across a spectrum of intensity. Choosing the right level depends on the severity of both conditions, the presence of medical risk, and the degree of social support available.
-
Outpatient programs (OP): Patients attend therapy sessions a few times per week while living at home. This works best for people with mild to moderate symptoms and a stable home environment.
-
Intensive outpatient programs (IOP): IOP typically involves 9–15 hours of structured treatment per week. Patients receive group therapy, individual counseling, and psychiatric support without residential placement. IOP is a strong option for people stepping down from higher levels of care.
-
Partial hospitalization programs (PHP): PHP provides 20–30 hours of clinical programming per week. It functions like a day program, offering near-residential intensity while allowing patients to return home each evening.
-
Residential programs: Patients live on-site and receive around-the-clock clinical support. Residential care is appropriate for people with severe symptoms, unstable housing, or a history of repeated relapse.
Across all levels, the most effective programs combine evidence-based therapy modalities with medication management. Trauma-focused CBT, dialectical behavior therapy (DBT), and contingency management are the most commonly used approaches. Each targets both the mental health and substance use components together, creating a synergistic effect that neither approach achieves alone.
Patients often seek programs that treat only their specific substance or only their mental health diagnosis. That instinct is understandable, but it leads to incomplete care. The right program treats the whole person, not a single diagnosis.
A holistic mental health treatment plan that incorporates psychiatric care, therapy, and lifestyle support gives patients the best foundation for sustained recovery. Continuous, long-term engagement with integrated care improves quality of life and housing stability over time. Recovery is not a short sprint. It is a sustained process that benefits from consistent, coordinated support.
Key Takeaways
Dual diagnosis treatment works best when both conditions are treated simultaneously by a unified clinical team from the very first day of care.
| Point | Details |
|---|---|
| Integrated care is the standard | SAMHSA’s fully integrated model produces the best retention, lowest relapse, and fewest hospitalizations. |
| Assessment must screen for both | DSM-5 interviews, PHQ-9, and GAD-7 together prevent diagnostic overshadowing and missed diagnoses. |
| No wrong door policy matters | Both conditions must be treated concurrently from day one, never sequentially. |
| Levels of care vary by need | OP, IOP, PHP, and residential programs each serve different severity levels and life situations. |
| Long-term engagement improves outcomes | Sustained integrated care leads to better quality of life and greater housing stability over time. |
Why I believe integrated care is the only honest path forward
I have spent years watching people cycle through treatment programs that were well-intentioned but structurally broken. A person would complete a 30-day residential program for alcohol use disorder, feel genuinely hopeful, and then return home to untreated depression that had been there the whole time. Within months, sometimes weeks, they were back where they started. The relapse was not a failure of willpower. It was a predictable consequence of incomplete care.
What I have come to believe, firmly, is that treating co-occurring disorders as separate problems is a kind of clinical fiction. The conditions do not live in separate compartments. They share biology, they share history, and they share the same nervous system. A treatment model that pretends otherwise is not just inefficient. It is actively harmful.
The patients I have seen make real, lasting progress are the ones who found programs willing to hold both realities at once. They had a psychiatrist and an addiction counselor who talked to each other. They had a therapy modality that addressed trauma without ignoring the substance use. They were never told to “get clean first” before their mental health would be taken seriously.
If you are researching options right now, the single most important question you can ask any program is this: “Do you treat both my mental health and my substance use from the very first day?” If the answer is anything other than yes, keep looking. You deserve care that sees all of you.
— Kabir
Mystic’s approach to integrated mental health and substance use care
Mystic brings psychiatric care and substance use treatment together under one clinical roof, so you never have to choose which part of yourself gets help first. The team at Mystic builds personalized treatment plans that address mental health and addiction as the interconnected conditions they are, drawing on evidence-based therapies, medication management, and whole-person healing practices. Whether you are exploring outpatient support or a more intensive level of care, Mystic’s integrated programs are designed to meet you where you are and move forward with you. Reach out to schedule a consultation and find out what a truly unified treatment plan looks like for your situation.
FAQ
What is the dual diagnosis definition?
Dual diagnosis refers to the co-occurrence of at least one mental health disorder and at least one substance use disorder in the same person. The term covers any combination of these conditions, not just two specific diagnoses.
How does dual diagnosis treatment work?
Dual diagnosis treatment works by addressing both the mental health and substance use disorders simultaneously through a single, coordinated clinical team. Integrated programs use shared records, joint medication management, and unified therapy goals to treat both conditions at once.
What are the signs of dual diagnosis?
Signs of dual diagnosis include persistent mood or anxiety symptoms that continue even during periods of sobriety, using substances to manage emotional distress, and a history of treatment that addressed only one condition without lasting results.
What therapy approaches are used in dual diagnosis programs?
Trauma-focused CBT, dialectical behavior therapy, and contingency management are the most widely used therapy modalities in dual diagnosis programs. These approaches target both mental health symptoms and substance use patterns at the same time.
Is long-term treatment necessary for dual diagnosis recovery?
Long-term, continuous engagement with integrated care produces the best outcomes for dual diagnosis recovery, including improved quality of life and greater housing stability. Recovery is an ongoing process, not a fixed endpoint.
Recommended

Mystic Health Blog








FAQs
1. Am I eligible for ketamine therapy?
2. Does insurance cover the cost of ketamine therapy?
3. How many ketamine treatments will I need?
We recommend two initial treatments to determine suitability and adjust dosage. After these sessions, additional treatments are available based on your progress and specific requirements.
