

Workflow for Cancer Pain Management: A Patient Guide
TL;DR:
- A structured workflow combines assessment, medication, and non-drug therapies to manage cancer pain effectively. Regular reassessment and early involvement of palliative care optimize outcomes and improve function. Patients and caregivers are active participants in tailoring the pain management plan.
A workflow for cancer pain management is a structured, stepwise process that combines medication, psychological support, and physical therapy to reduce pain and restore daily function. The clinical term for this approach is multimodal pain management, and it is the gold standard recognized by the World Health Organization (WHO), the National Comprehensive Cancer Network (NCCN), and major oncology societies worldwide. Getting this process right matters deeply. Pain is one of the most common and distressing symptoms in cancer, and a clear cancer pain control process gives you and your care team a shared map to follow. This guide walks through every stage of that map, from first assessment to long-term adjustments, so you can show up for yourself and for the people you love.
What are the core components of a cancer pain management workflow?
Effective pain relief protocols for cancer begin with understanding what kind of pain you are dealing with. Pain in cancer falls into three main types: neuropathic (nerve-related burning or shooting sensations), somatic (localized aching from tissue or bone), and visceral (deep, diffuse pressure from organs). Identifying the type shapes every treatment decision that follows.

Assessment tools and team roles
Clinicians use validated pain scales, such as the Numeric Rating Scale (0–10) and the Brief Pain Inventory, to measure intensity and functional impact at every visit. These tools capture not just how much something hurts, but how pain affects sleep, mood, and movement. A multidisciplinary care team typically includes an oncologist, palliative care specialist, psychologist, physical therapist, and pharmacist. Each role fills a gap that no single provider can cover alone.
Medications used in the workflow
Gold-standard cancer pain management combines long-acting opioids for baseline control with short-acting opioids for breakthrough episodes, using dose titrations of 25–50% every 24–48 hours. Adjuvant medications, including antidepressants, anticonvulsants, and corticosteroids, address specific pain types that opioids alone do not fully control. Knowing the difference between maintenance dosing and rescue dosing is one of the most practical things a caregiver can learn early.
Non-pharmacologic options
Non-pharmacological interventions such as cognitive behavioral therapy (CBT) and mindful pacing work alongside medications to reduce overall drug requirements. Physical therapy, acupuncture, and rehabilitation exercises address the body’s physical response to pain. These are not optional add-ons. They are core parts of the workflow from day one.
Pro Tip: Ask your care team to document your pain type at the first visit. Knowing whether your pain is neuropathic, somatic, or visceral helps every provider on your team make faster, better decisions.
How do you execute the stepwise cancer pain management workflow?
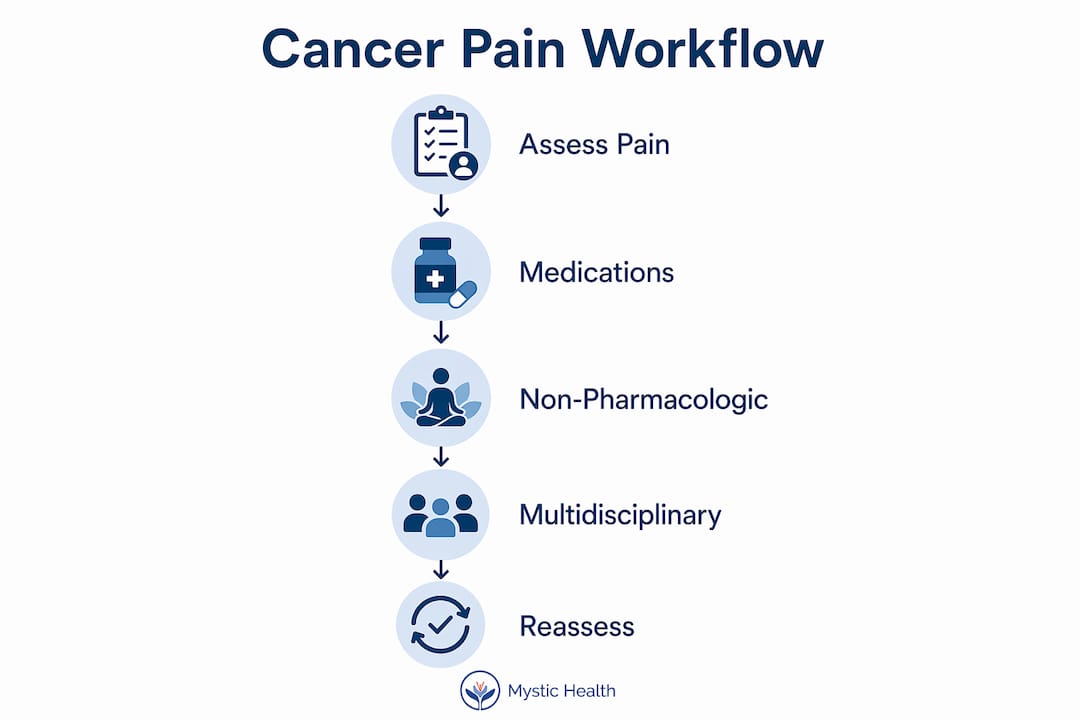
The cancer pain control process follows a clear sequence, though it is not rigid. Clinicians adapt each step based on how you respond.
-
Initial evaluation (30–60 minutes). Pain specialist evaluations cover pain location, severity, mechanism, sleep disruption, and daily function before any treatment begins. This session is the foundation. Skipping it leads to mismatched treatments.
-
Start pharmacologic therapy. The WHO analgesic ladder provides a useful conceptual framework, but clinicians often skip steps to avoid delays when pain is moderate to severe. Starting a strong opioid directly is appropriate and common in significant pain cases.
-
Titrate to effect. Dose increases of 25–50% every 24–48 hours are standard until pain is controlled. Small, cautious increases that leave pain unmanaged are not safer. They just prolong suffering.
-
Add rescue dosing. Breakthrough pain requires a separate immediate-release opioid at roughly 10–20% of the total 24-hour baseline opioid dose. This is distinct from the maintenance medication and must be tracked separately.
-
Integrate non-drug therapies. CBT, physical therapy, and mindfulness practices enter the workflow at this stage, not later. Early integration reduces the total opioid load needed over time.
-
Reassess at every clinical encounter. Pain management is dynamic and requires iterative reassessment tied to cancer progression and treatment effects. A pain plan that worked last month may need adjustment today.
Pro Tip: Keep a simple daily pain log, rating your pain at the same time each day and noting what helped or did not. This gives your care team real data instead of memory-based estimates.
What holistic and multidisciplinary strategies improve cancer pain outcomes?
Medication alone rarely delivers the best results. Modern pain workflows now require holistic strategies including psychological support, physical therapy, and interventional procedures as standard components, not afterthoughts.
Psychological approaches make a measurable difference. CBT teaches patients to reframe pain-related thoughts and reduce the anxiety that amplifies physical pain signals. Mindfulness-based stress reduction gives you tools to stay present without being consumed by discomfort. Therapy for cancer patients also addresses grief, fear, and the emotional weight that caregivers carry alongside their loved ones.
Physical therapies keep the body moving safely. Rehabilitation specialists design exercise programs that account for fatigue, bone fragility, and post-surgical limitations. Movement modification, gentle stretching, and graded activity prevent the deconditioning that makes pain worse over time.
For pain that does not respond to oral medications, interventional procedures offer relief. Nerve blocks, neurolysis, and intrathecal drug delivery target specific pain pathways directly. These are not last resorts. They are appropriate tools when the pain mechanism calls for them.
Early palliative care integration is one of the most impactful steps in the entire workflow. Palliative care addresses complex symptom management and whole-person needs, and it is not synonymous with end-of-life care. Patients who receive palliative care early report better pain control and reduced use of intensive medical interventions.
Patient and caregiver education belongs in this section too. When you understand your medications, their timing, and their side effects, you become an active partner in the care plan rather than a passive recipient.
How do you troubleshoot and personalize your cancer pain plan?
Even a well-designed plan needs adjustment. Pain changes as cancer evolves, and the workflow must change with it.
-
Manage breakthrough pain proactively. Rescue doses of 10–20% of the baseline opioid should be available and clearly prescribed before breakthrough episodes occur, not after. Waiting until pain spikes to ask for rescue medication is a common and preventable mistake.
-
Address opioid side effects early. Constipation is nearly universal with opioid use and requires a scheduled bowel regimen from the start. Sedation often improves within a few days but should be reported if it persists or worsens.
-
Consider opioid rotation. When one opioid causes intolerable side effects or loses effectiveness, switching to a different opioid at an equianalgesic dose often restores both relief and tolerability. This is a standard clinical tool, not a sign of failure.
-
Shift the goal from elimination to function. Clinicians now target function-optimized pain management rather than complete pain freedom. The realistic benchmark is: can you sleep, eat, and engage with the people you love? That is the measure that matters.
-
Keep communication open. Feedback loops between patients, caregivers, and the care team are what make the workflow actually work. Report changes in pain character, not just intensity. A shift from aching to burning may signal a new nerve involvement that needs a different treatment approach.
“Pain management is an iterative process. It requires consistent reassessment and adjustment linked to cancer progression and treatment effects.” — Update on Cancer Pain Management
Key takeaways
A structured, multimodal workflow is the most effective approach to cancer pain management, combining medication, psychological care, and physical therapy with regular reassessment at every stage.
| Point | Details |
|---|---|
| Start with thorough assessment | Identify pain type, severity, and functional impact before choosing any treatment. |
| Use rescue dosing correctly | Breakthrough pain needs a separate immediate-release opioid at 10–20% of the daily baseline dose. |
| Integrate non-drug therapies early | CBT, mindfulness, and physical therapy reduce opioid needs and improve quality of life from the start. |
| Involve palliative care early | Early palliative care improves pain control and whole-person support, not just end-of-life care. |
| Reassess consistently | Pain plans must be updated at every clinical encounter as cancer and treatment evolve. |
What I’ve learned about cancer pain that most guides won’t tell you
I’ve worked alongside patients and caregivers navigating cancer pain for years, and one pattern stands out above all others: people wait too long to ask for help. They minimize their pain because they do not want to seem difficult, or because they believe suffering is just part of the process. It is not.
The shift that changes everything is moving from “how do I endure this?” to “how do I function through this?” That reframe is not just philosophical. It is clinical. Functional improvement, not pain elimination, is the realistic and meaningful goal. When you aim for the ability to sleep through the night or share a meal with your family, the entire care plan becomes more focused and more achievable.
The other thing I see underestimated constantly is the power of non-medication strategies. Patients often arrive convinced that only stronger opioids will help. But CBT, mindfulness, and physical therapy are not soft alternatives. They are evidence-based tools that change how the nervous system processes pain. Combining them with medication produces results that neither approach achieves alone.
Caregivers, this applies to you too. Your understanding of the pain plan, your ability to track symptoms and communicate them clearly, and your presence in appointments all shape outcomes. You are not a bystander. You are part of the team.
Finally, do not wait for a crisis to involve palliative care. Early involvement is one of the most consistently supported recommendations in oncology, and it gives patients more space to breathe, more control, and more time focused on living rather than just managing.
— Kabir
How Mystic supports patient-centered cancer pain care
Living with cancer pain is one of the hardest things a person can face. You deserve a care team that sees the whole picture, not just the symptom.
Mystic brings together integrative medicine programs that blend pharmacologic treatment, psychological therapy, and palliative support into one coordinated plan. Whether you are a patient working through a new diagnosis or a caregiver trying to understand your loved one’s options, Mystic’s programs are built around your specific needs. The team at Mystic draws on evidence-based modalities including ketamine-assisted therapy, mindfulness, and supportive counseling to address pain at every level. Learn more about Mystic’s cancer support resources and find a path forward that feels right for you.
FAQ
What is a workflow for cancer pain management?
A workflow for cancer pain management is a structured, stepwise process combining assessment, medication, non-drug therapies, and regular reassessment to control pain and improve daily function. It follows guidelines from organizations like WHO and NCCN.
How is breakthrough pain different from regular cancer pain?
Breakthrough pain is a sudden spike in pain that occurs despite stable baseline medication. It requires a separate immediate-release opioid, typically dosed at 10–20% of the total daily baseline opioid intake.
When should palliative care be involved in cancer pain management?
Palliative care should be involved early in the cancer diagnosis, not only at end of life. Early integration improves pain control, reduces intensive care use, and supports whole-person wellbeing.
Do non-medication therapies actually reduce cancer pain?
Yes. CBT, mindfulness, and physical therapy work alongside medications to reduce opioid requirements and improve quality of life. They address the psychological and physical dimensions of pain that drugs alone cannot fully reach.
How often should a cancer pain plan be reassessed?
Pain plans should be reassessed at every clinical encounter. Because cancer and its treatments change over time, the pain management approach must be updated consistently to stay effective.
Recommended

Mystic Health Blog








FAQs
1. Am I eligible for ketamine therapy?
2. Does insurance cover the cost of ketamine therapy?
3. How many ketamine treatments will I need?
We recommend two initial treatments to determine suitability and adjust dosage. After these sessions, additional treatments are available based on your progress and specific requirements.
